Using Technology to Build the Capacity of Health Workers in India
April 6th, 2018 | news
The performance of health personnel is crucial to improving facility service delivery and overall quality of care. In order to enhance personnel performance throughout its health system, India’s Ministry of Health and Family Welfare (MoHFW) recently shifted from traditional supervisory mechanisms to supportive supervision. Supportive supervision is a facilitative approach that promotes mentorship, joint problem-solving, and communication between supervisors and supervisees.
Supervisory officials at the country’s block, district, division, and state levels support and guide a massive cohort of frontline workers, including over 200,000 Auxiliary Nurse Midwives. The MoHFW has worked to streamline supportive supervision across the health system by developing a checklist with performance indicators in four thematic areas. This form of mentorship is a new concept for India’s vast health network, and there are several challenges and potential opportunities in its institutionalization. One opportunity is electronically structuring supportive supervision and its monitoring, which could create uniform protocols and better-informed decision-making for improved performance.
With the support of the Bill & Melinda Gates Foundation (BMGF), JSI India partnered with the Government of India to develop software that would facilitate the recording and follow-up of supervisory support. The software is designed to engage supervisory health staff, development partners, and other stakeholders to improve the public health system and quality of health care services through a systematic, technology-based approach.
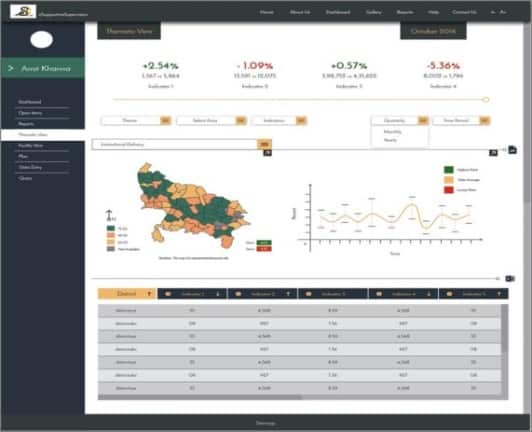
The software, which works on various devices and in online and offline modes, aids supervisory staff in planning facility visits, analyzing facility status, developing subsequent plans of action, delegating action items, and disseminating facility assessments. It facilitates performance analysis through a number of filters, including thematic area, geographic breakdown, and individual performance. To track supervision and improvement, the software displays:
JSI facilitated the formation of the project’s Technical Support Group (TSG) with representatives from the National Health Systems Resource Centre, BMGF, Access Health, IPE Global, and UNICEF. The TSG informed and approved the development of the software in consultation with the MoHFW. The software was piloted in one district in each of these four states: Varanasi (Uttar Pradesh), Jashpur (Chhattisgarh), Krishnagiri (Tamilnadu), and Sangareddy (Telangana).
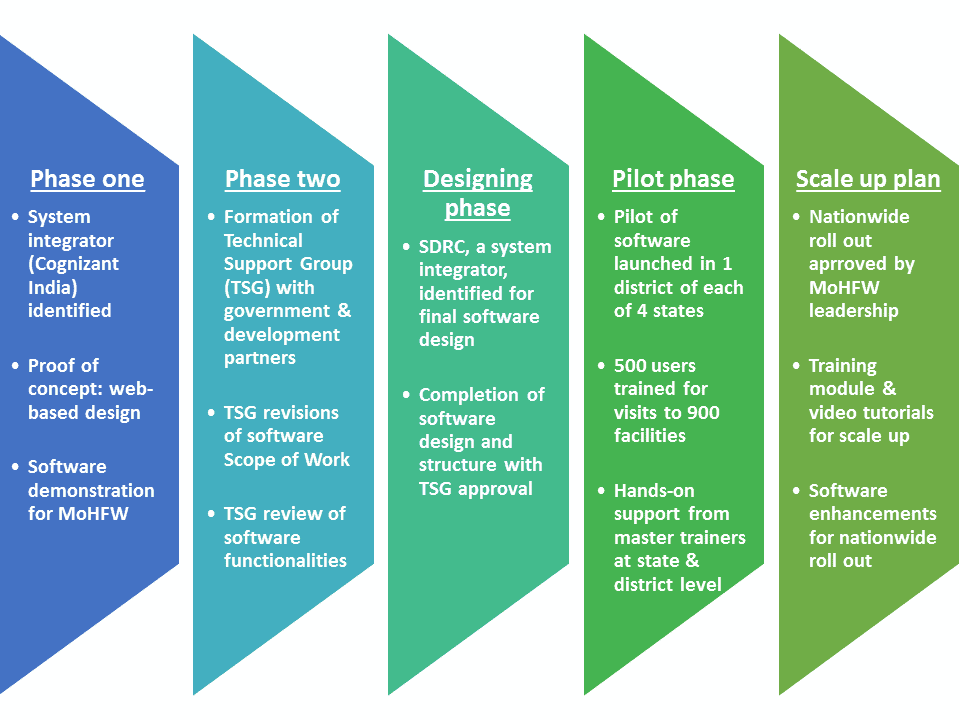
Findings from the pilot showed that the software is scalable and generated insights to improve the tools. The pilot included over 500 trained users among supervisory staff in health departments at the national, state, district, and sub-district levels. These users tested the software at 900 facilities from districts to sub-health centers, generating more than 1,900 action items.
While the pilot was successful and showed great potential for the electronic supportive supervision approach, there were some challenges that led to important lessons learned. One key finding was that while trainings were designed to introduce the new supportive supervision software, many participants had never received training on supportive supervision as a concept. If the system is to be scaled, it will be important to include focused training time on supportive supervision processes before diving into the software. Users also had difficulties adjusting to the software in real-life settings post-training, pointing to a need for increased hands-on practice in future trainings on the software.
The combined leadership of BMGF, JSI India, and the MoHFW led to the success of the software in health settings. The MoHFW is pleased with the results of the pilot. The partnership is identifying what is required to reach national scale, including cost, institutionalization within the MoHFW, and training plans. Throughout the process, we hope to continue to instill confidence in users and maintain MoHFW support in pursuing this technology to support health personnel and improve health service delivery across India.
We strive to build lasting relationships to produce better health outcomes for all.




