Creating an Information Revolution Model: Digital Health Activity’s Approach for Implementation at Scale
June 9th, 2021 | viewpoint
The Ministry of Health (MOH) in Ethiopia has invested in health information systems (HISs) development under the HSTP and, more specifically, the Information Revolution Roadmap (IRR). The Digital Health Activity (DHA) contributes to the implementation of the country’s IRR, which supports the goals of improving the quality of health services, improving people’s quality of life, and building a sustainable health care system by using data for decision making.
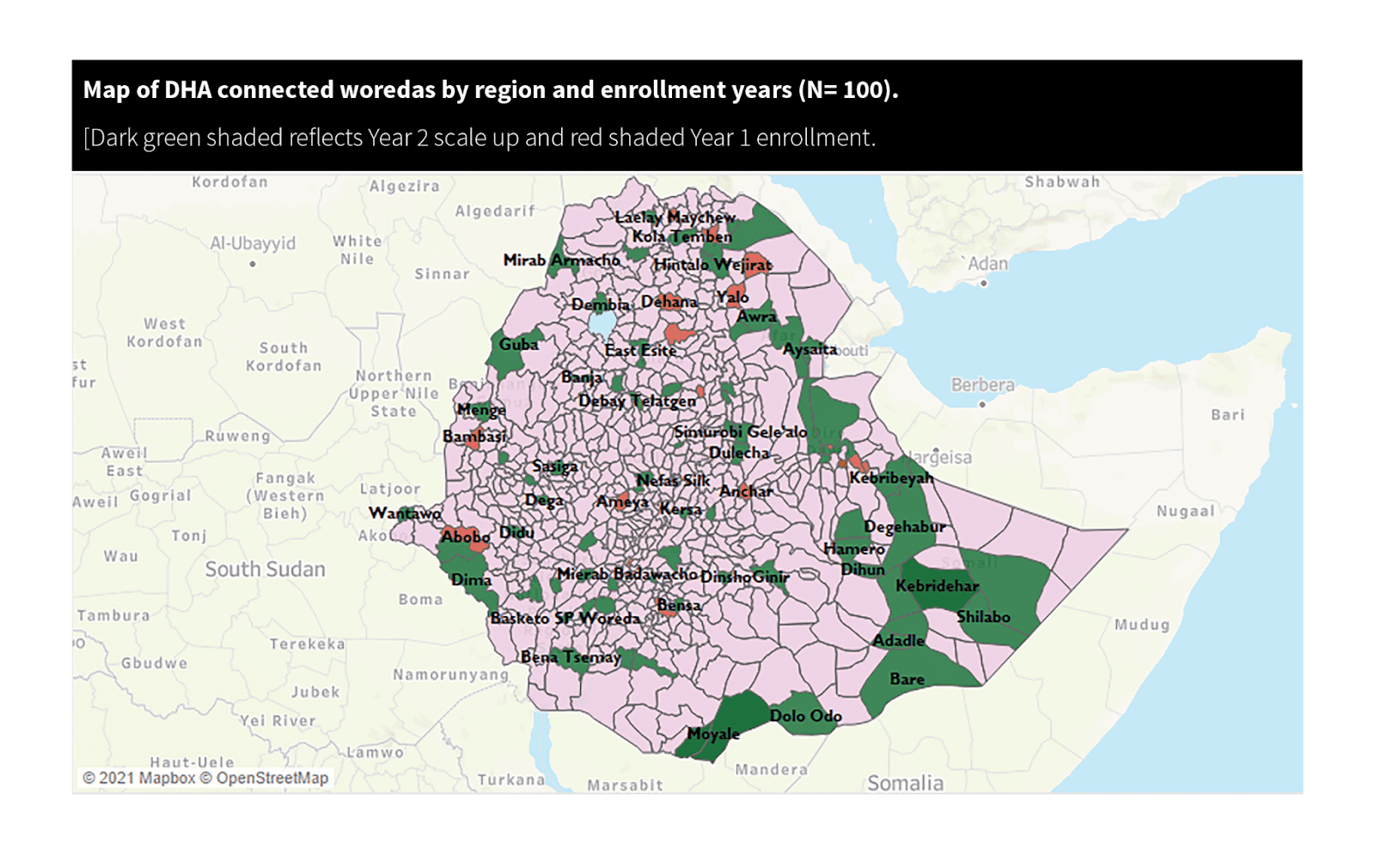
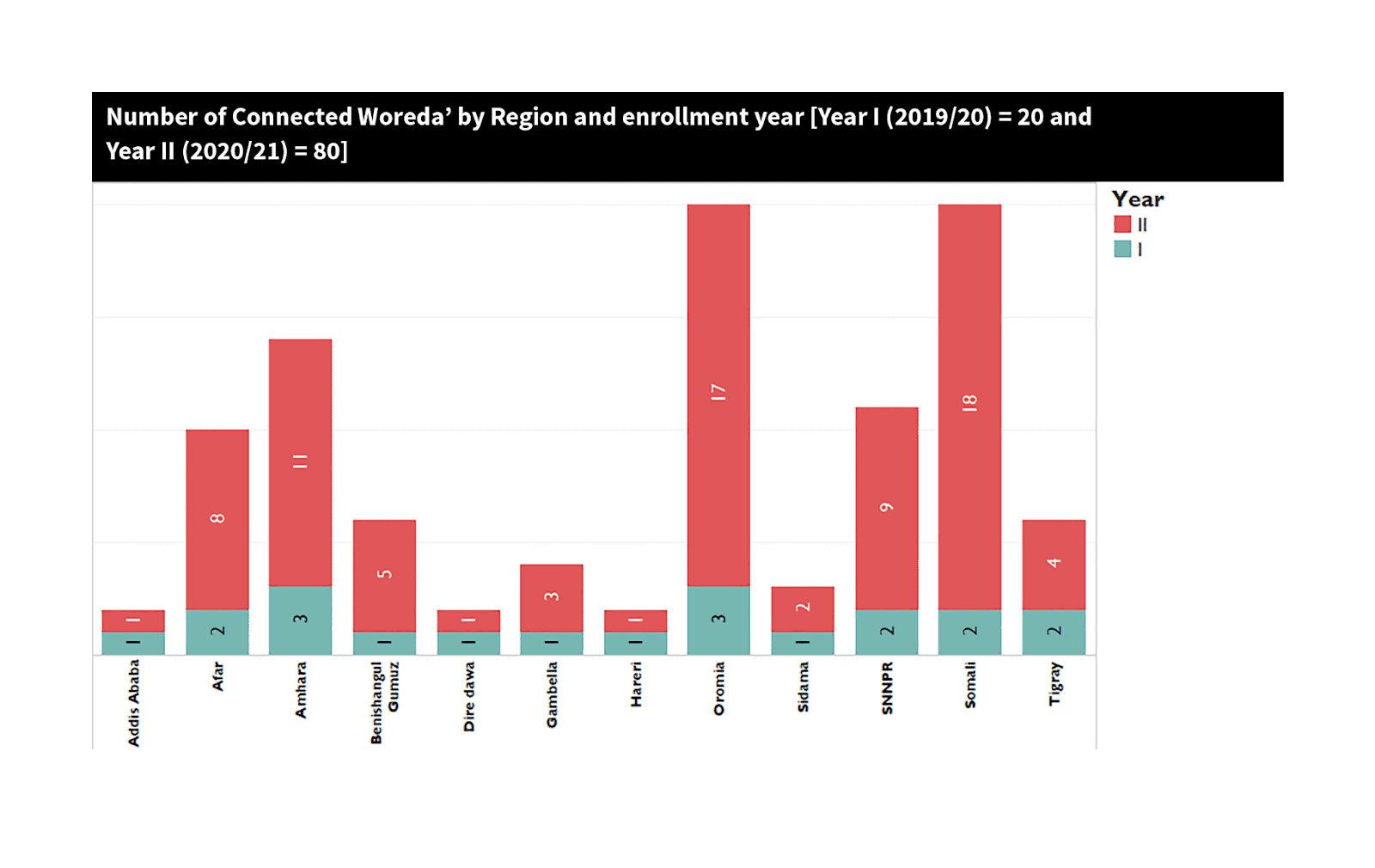
To operationalize the implementation of the IRR at woreda and health facility levels, MOH developed and started the Connected Woreda (CW) strategy, which aims to strengthen HIS infrastructure and capacity, improve health data quality, and encourage data use at the point of service delivery. As a major component of the Activity’s major objectives—transforming the culture of information use—DHA is directly supporting the implementation of the CW strategy across all regions. DHA supports 100 (roughly 10%) of the country’s woredas to improve data quality, data use, and HIS infrastructure. DHA uses the principle of collaborative effort targeting sustainability of CW implementation.
 This started with a joint identification of woredas through setting criteria, mapping partners, and allocating more resources to developing regions. Baseline data collection using a national tool was the starting point of implementation, coupled with dissemination of baseline benchmarks to stratify the woredas, health centers, hospitals, and health posts. All stakeholders agreed on the baseline grading and prepared tailored interventions. Additionally, regional health bureaus (RHB) and zones participated in a two-day meeting to ensure that implementation is monitored and evaluated based on agreed targets. All implementations are RHB-led with DHA support.
This started with a joint identification of woredas through setting criteria, mapping partners, and allocating more resources to developing regions. Baseline data collection using a national tool was the starting point of implementation, coupled with dissemination of baseline benchmarks to stratify the woredas, health centers, hospitals, and health posts. All stakeholders agreed on the baseline grading and prepared tailored interventions. Additionally, regional health bureaus (RHB) and zones participated in a two-day meeting to ensure that implementation is monitored and evaluated based on agreed targets. All implementations are RHB-led with DHA support.
The CW interventions ranged from review meetings to understand the concepts of data use to on-the-job training, supportive supervision, and mentorship. We have learned that joint intervention planning and implementation ensures ownership, efficient use of resources, and prioritization of activities according to regional plans and sustainability strategies.
One of the major activities under the connected woreda implementation is mentorship to woreda health offices and health facilities. DHA’s mentorship approach is based on a guideline developed by the MOH in 2019. Through the mentorship approach, DHA has been supporting the CW initiative in improving the status of woredas in the CW pathway. DHA mentors are high-caliber HIS practitioners who have experience mentoring and coaching across Ethiopian HIS.
DHA used the peer coaching approach to develop the capacity of mentors among staff and RHBs, zonal health departments (ZHD), and woreda health office staff. Mentorship orientation included the MOH mentorship guideline printed checklists and an open data kit (ODK) form that equips the mentees to fill the identified skill gaps. DHA trained data use champions in each area of its operation through off-the-job trainings, and is developing online modules to further build mentor capacity. DHA staff are conducting quarterly mentorship for each health facility in the CW via face-to-face and distant support.
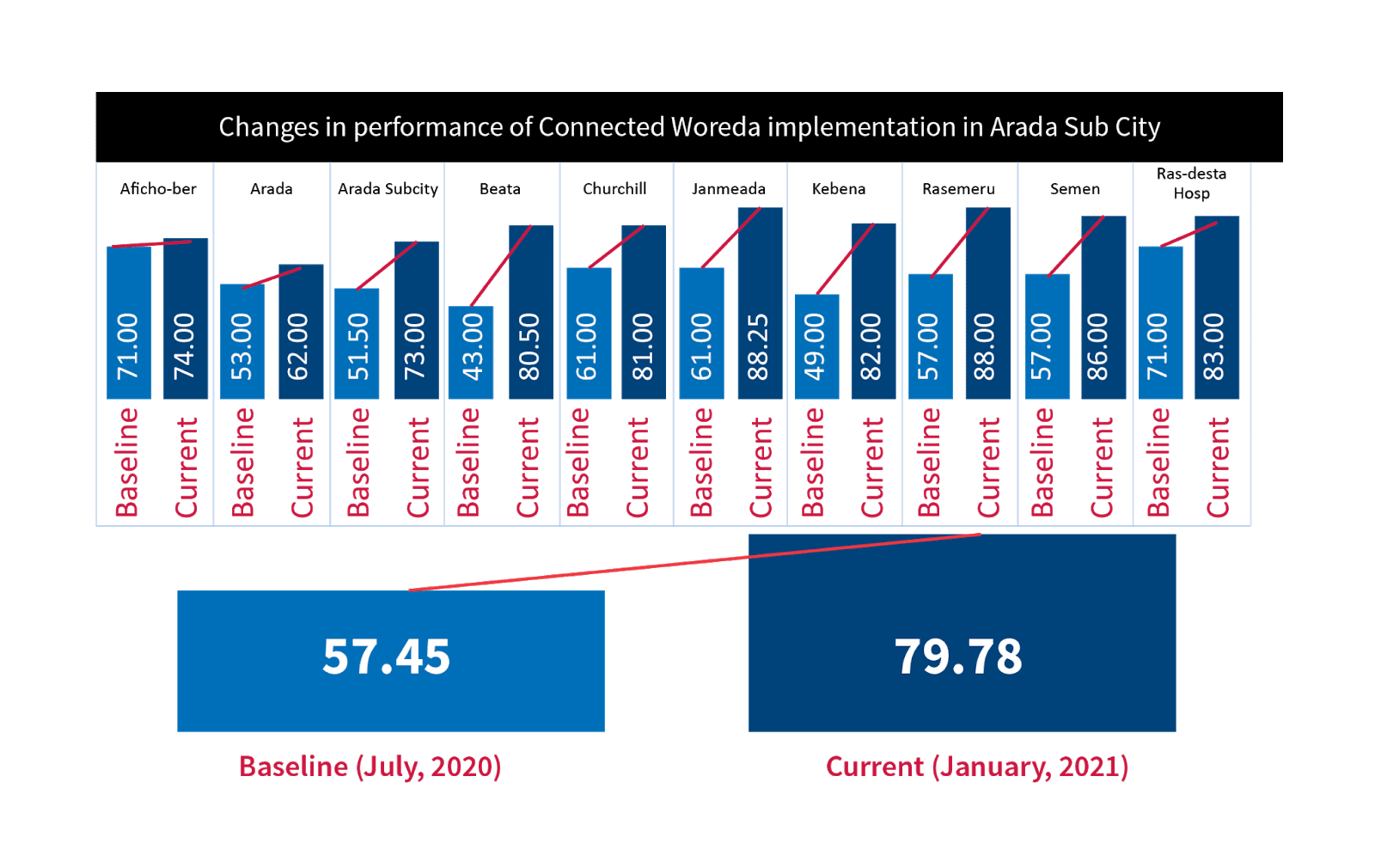
The interventions so far indicate substantial gains in baseline benchmarks. For instance, a comparison of baseline and self assessment in Arada sub-city in Addis Ababa indicated that facilities have improved significantly, from 59 to 80 percent since the start of the intervention.
The following are the major approaches in which DHA has been actively involved:
Site visits involve in-person interaction and observation of the strengths and weaknesses of the HIS implementation and data quality. Visits are considered the best mentoring model because they facilitate skill transfer and technical assistance in recording, reporting, and performance management team (PMT) revitalization. They also provide opportunities for information and communications technology (ICT)-related troubleshooting across products (DHIS2, electronic medical records (EMR), eMCS, Dagu, mBrana, and HealthNet related problems).
Most of the time, DHA field officers stay 2–3 days at each facility to make sure mentees understand concepts and prepare action plans.
In developing countries, the choice of ICT-based remote mentoring is contingent upon many conditions, for example, availability and functionality of ICT infrastructure and the presence of a particular ICT literate mentee. ICT-based mentoring has been especially practical and accommodating during COVID-19. As we strengthen infrastructure issues, we will learn more about its advantages.
This cost-effective and efficient approach requires mobile network coverage and a mobile phone capable of conference calling. DHA field staff have been using this approach to strengthen the mentorship program they established at health facilities. It is helpful for tracking progress on agreed action plans between and among different administrative units.
Health facilities and woredas have shown immense progress in HIS structures, functions, and resources; data quality; evidence-based decision making, and strengthened PMTs. For example, in Anchar woreda in Oromia Region, data quality has improved by sustaining greater than 95% content completeness in the five health centers for the last six months and all have conducted lot quality assurance sampling (LQAS) in the same period, and the woreda health office has been conducting regular routine data quality assessments (RDQA).
Written by Biruk Tensou and Abiy Semunigus
We strive to build lasting relationships to produce better health outcomes for all.



