Simplicity in Solutions
July 23rd, 2021 | story
This blog was originally posted by the Boost Community in July 2021.
Along the western slopes of the imposing Himalayas lies one of India’s northernmost states – Himachal Pradesh, which in Hindi means the “snow-laden province.” Within this mountainous region lies Saroa, a village in Bagsaid Block of Mandi District, where Sandeepa Kumari serves as an Auxillary Nurse Midwife (ANM) in the Health Sub-Center, which caters to a population of just over three thousand people. Sandeepa is one of over 200,000 ANMs who serve at the frontlines of one of the largest immunization programs on the planet. Sandeepa is tasked with managing immunization for the area’s children and pregnant women through both the Saroa and Tandi Sub-Centers. With multiple demands on her time, planning for immunization is fundamental to effectively serving the mothers and children in her catchment where the terrain is difficult to traverse.
Every six months, Sandeepa updates a microplan for immunization activities in her assigned villages. The first step towards setting immunization targets is a head-count survey in the assigned catchment area/village and updating the microplan which enables births to be systematically tracked. However, Sandeepa is not alone in this endeavor. She works closely with two other cadres of frontline workers.The first is the Accredited Social Health Activist, popularly known as the ASHA. This is a community volunteer who serves between 800 to 1000 people, or a village, and acts as a crucial link between the ANM at the health facility and the community. ASHAs are responsible for driving demand for immunization, encouraging deliveries in facilities and ensuring adherence to mother and child health best practices. In this mountainous region that suffers from severe winters, having the ASHA on hand in the villages to remind and encourage mothers of the value of vaccination even if it means a five-kilometer trek in the cold winter months has been critical for ensuring vaccine uptake. The third leg to this ‘sturdy stool’ is the Anganwadi Worker (AWW), the most grassroots representative of the Ministry of Women and Child Development, a testament to the fact that health is not the sole responsibility of one entity – the Ministry of Health and Family Welfare. The AWW’s main role is to support improved nutritional status among infants, children and lactating mothers, which in recent years has extended to adolescent health. Every village in India has at least one Anganwadi center housed in a courtyard shelter. These centers are focal points for the implementation of all the health, nutrition and early learning initiatives under the Integrated Child Development Services program (ICDS). The AWWs regular interaction with fellow villagers also allows for informal conversations around the need for immunization, ultimately reducing vaccine hesitancy and myths. This combination of support is commonly known as the Triple A, which is the backbone of health delivery at the grassroots level.
While the ASHAs and AWWs are active in the community, they rely on information that is generated from the ANM at the Health Center. Responsible for the two sub-centers, Sandeepa’s catchment extends to several villages in the area. Her contact with mothers though remains facility-based, meaning that her success relies on the ASHAs and AWWs in her location to ensure that mothers go to the facility when they need to.
A valuable aid in this planning is the Tracking Bag.
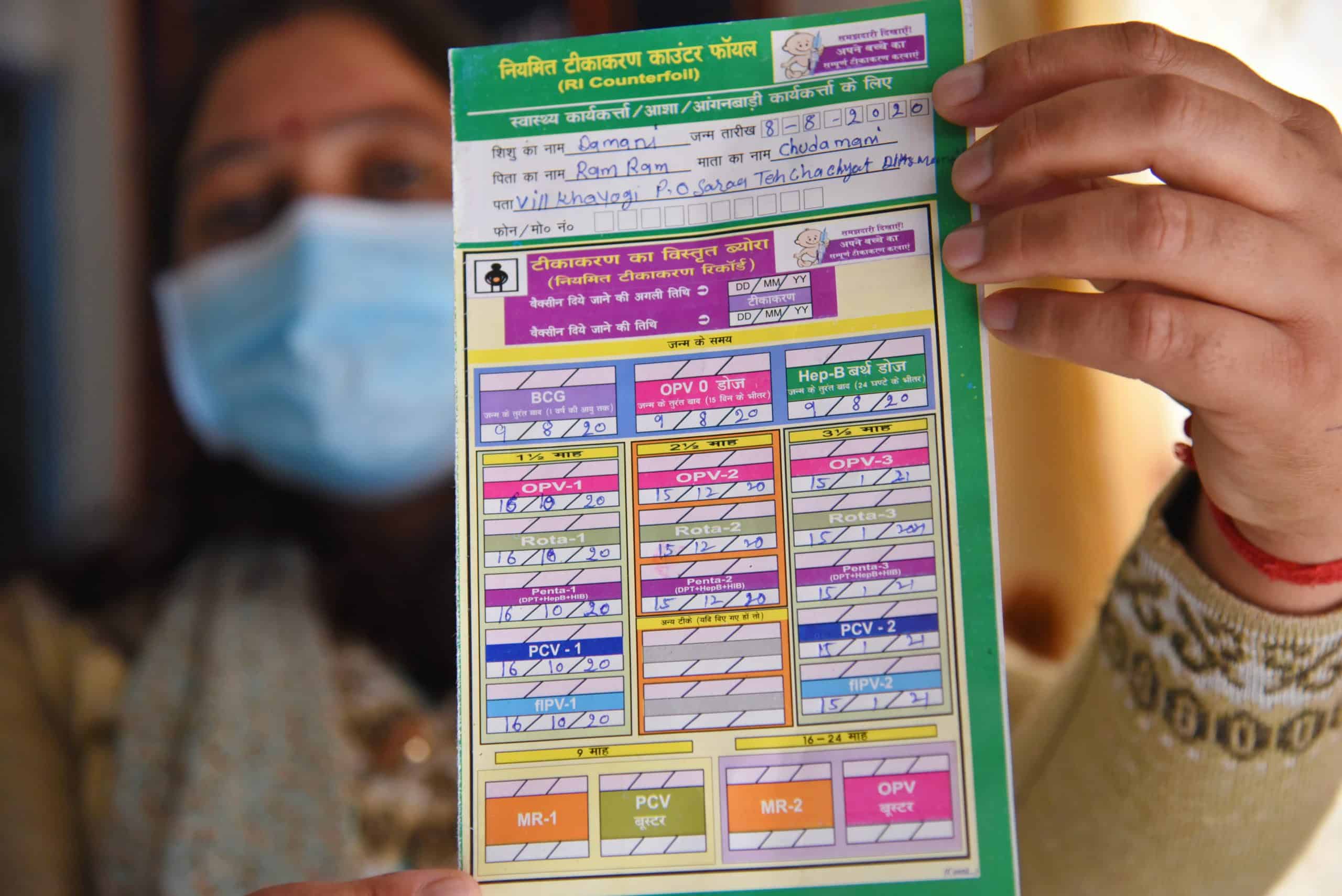
This simple tool has been a gamechanger in managing and planning for visits and ensuring immunization of children is completed by the three health functionaries. Each center hosts one vaccination day a month and every pregnant woman is provided with a Mother and Child Protection (MCP) Card during their antenatal visit. The MCP card has a main section and a detachable counterfoil. The main section is given to the caregiver to be brought to the next vaccination session, which could be during outreach or at the sub-center. The counterfoil is retained at the sub-centre for record purposes. After each vaccination session, all vaccine-related information is updated on the main card as well as on the counterfoil.

Each tracking bag has 12 pockets one for each month of the year as well as two extra pockets – one for children who have passed away or left the area and another for those who are fully immunized. By the end of the monthly vaccination day, all the Mother and Child Protection (MCP) Cards are placed into the corresponding month’s pockets for the next visit.
After each visit, both segments are updated with the relevant antigens that have been administered and the counterfoil is placed in the pocket corresponding to the month when the child is expected for the next round of vaccinations. The Tracking Bag has 12 pockets – one for each month of the year- as well as two extra pockets, the first for children who have passed away or left the area and the second for those who are fully immunized.
By the end of the monthly vaccination day, all the cards have been placed into the corresponding month’s pockets for the next visit. Together, Sandeepa and the resident ASHA examine the current month’s pocket to see who didn’t arrive as expected and make a list of those due the following month. With these two lists – the defaulters and “due list”, the ASHA has her plan in place. Defaulters are immediately identified, allowing each ASHA to follow up on children from her village who missed their appointment. Additionally, in the run-up to the next vaccination day, she goes around from house to house reminding parents of the upcoming visit. This targeted, name-based focus has been instrumental in attracting previously unvaccinated children, reducing defaulters, and achieving high vaccination completion rates.
The Tracking Bag may seem like a somewhat simple tool; however, its uncomplicated and straightforward process is much less cumbersome than managing a register, reduces the chance of mistakes in logging information and provides instant clarity for those whose work is defined by the data it holds.
Each ANM needs to deliver a full complement of vaccines, which includes over seven visits to each under-5 child in their care. Against this backdrop the value of the Tracking Bag becomes clear. Moreover, in geographies with limited connectivity, where technology-based management tools may not be a solution for monitoring, low-tech tools such as the Tracking Bag still have a vital role to play.
In the last decade the percentage of surviving infants who received the third dose of DTP-containing vaccine has risen by almost ten percent to 91% in India.
This Bright Spot story was nominated by Ajai Kumar, Team Lead, Strategic Communication with the Immunization Technical Support Unit in New Delhi, India. Ajai hopes that this story can demonstrate how simple tools can be instrumental assets in serving previously unvaccinated children, lowering defaulter rates and enhancing immunization tracking, especially in geographies with low connectivity, internet penetration and difficult terrain
We strive to build lasting relationships to produce better health outcomes for all.




